Obgyn History Template
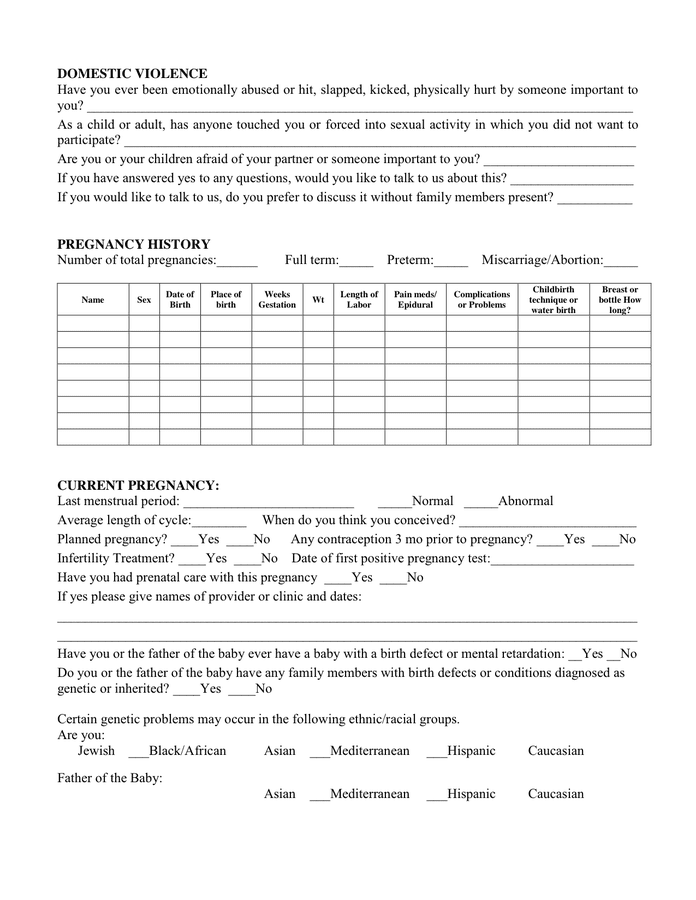
Obgyn History Template - If your menstrual periods are regular; Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we leave a secured voice mail? If so, what was the diagnosis and when? Up to 40% cash back edit, sign, and share ob gyn history and physical sample online. Gynaecological history taking opening the consultation 1 wash your hands and don ppe if appropriate 2 introduce yourself to the patient including your name and role 3. Have you ever had a. Were you on birth control when you got pregnant? Have you ever been diagnosed with a medical or psychological condition? (03/11) page 1 of 4 mrn: Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev. Have you ever been diagnosed with a medical or psychological condition? If you have previously filled out the updated version,. Were you on birth control when you got pregnant? A thorough woman's health and social history was taken including menstrual, sexual, obstetric, medical, surgical, family, and social histories. Up to 40% cash back edit, sign, and share ob gyn history and physical sample online. Relevant details were obtained to guide the. The document outlines a comprehensive patient assessment. Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. The document outlines a comprehensive patient assessment. Have you ever been diagnosed with a medical or psychological condition? Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev. If your menstrual periods are regular; Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology & infertility name: Have you ever had a. Gynaecological history taking opening the consultation 1 wash your hands and don ppe if appropriate 2 introduce yourself to the patient including your name and role 3. Relevant details were obtained to guide the. Up to 40% cash back edit, sign, and share ob gyn history and physical sample online. If you have previously filled. If you have previously filled out the updated version,. If your menstrual periods are regular; Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Have you ever had a. This document outlines the components of an obstetrics and gynecology history taking, including sections on introduction/demographics, menstrual history, present pregnancy history, past. This document outlines the components of an obstetrics and gynecology history taking, including sections on introduction/demographics, menstrual history, present pregnancy history, past. A thorough woman's health and social history was taken including menstrual, sexual, obstetric, medical, surgical, family, and social histories. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Up to 40%. If you have previously filled out the updated version,. Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can. The document outlines a comprehensive patient assessment. Obstetric history taking opening the consultation 1 wash your hands and don ppe if appropriate 2 introduce yourself to the patient including your name and role 3 confirm. What day was your pregnancy test first positive? This document outlines the components of an obstetrics and gynecology history taking, including sections on introduction/demographics, menstrual. Have you ever been diagnosed with a medical or psychological condition? Obstetric history taking opening the consultation 1 wash your hands and don ppe if appropriate 2 introduce yourself to the patient including your name and role 3 confirm. A thorough woman's health and social history was taken including menstrual, sexual, obstetric, medical, surgical, family, and social histories. Gynaecological history. Obstetrical history including abortions & ectopic (tubal) pregnancies. What day was your pregnancy test first positive? Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology & infertility name: Relevant details were obtained to guide the. Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev. Have you ever been diagnosed with a medical or psychological condition? Simplify patient intake with a customizable obgyn history form. What birth control method(s) do you currently use? This document outlines the components of an obstetrics and gynecology history taking, including sections on introduction/demographics, menstrual history, present pregnancy history, past. Medical history questionnaire department of obstetrics & gynecology division of. The document outlines a comprehensive patient assessment. Have you ever had a. If so, what was the diagnosis and when? Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology & infertility name: Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted. Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. A thorough woman's health and social history was taken including menstrual, sexual, obstetric, medical, surgical, family, and social histories. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we leave a secured voice mail? Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology & infertility name: Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev. If you have previously filled out the updated version,. The document outlines a comprehensive patient assessment. This document outlines the components of an obstetrics and gynecology history taking, including sections on introduction/demographics, menstrual history, present pregnancy history, past. Have you ever been diagnosed with any of the following? What birth control method(s) do you currently use? If your menstrual periods are regular; What day was your pregnancy test first positive? If so, what was the diagnosis and when? Relevant details were obtained to guide the. Were you on birth control when you got pregnant?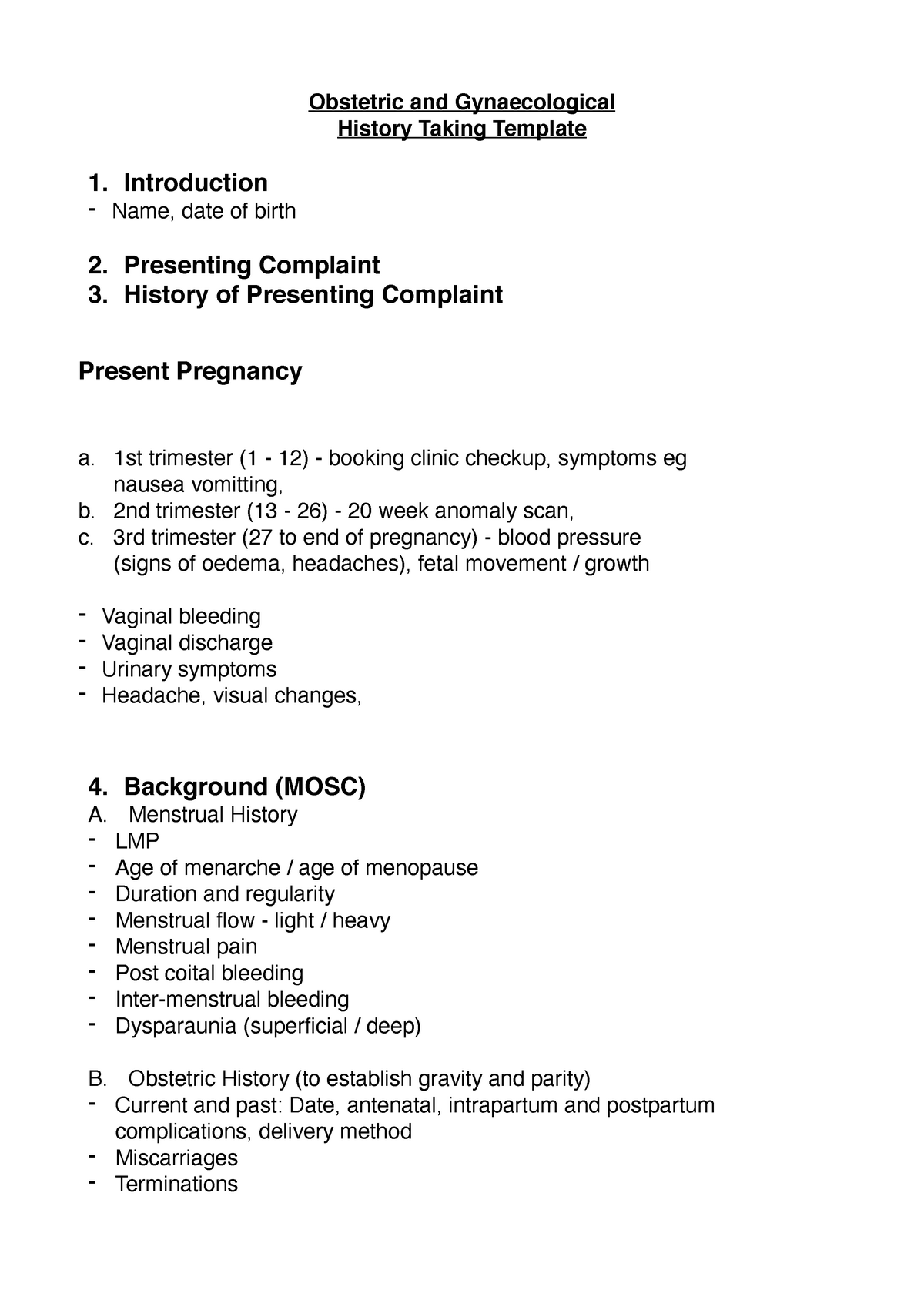
History Taking Template
Obgyn History Template
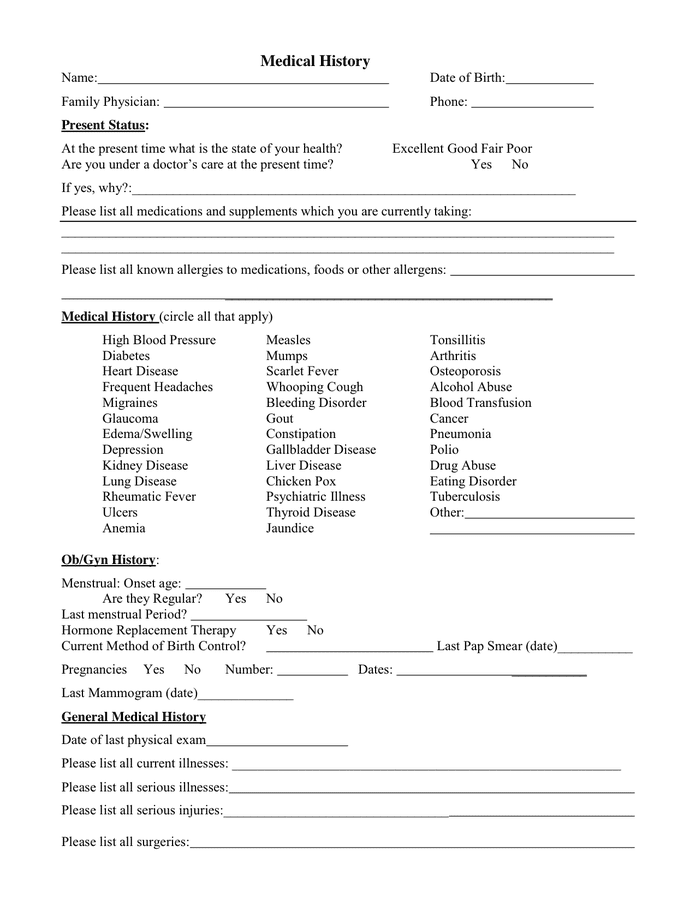
Medical History Form in Word and Pdf formats
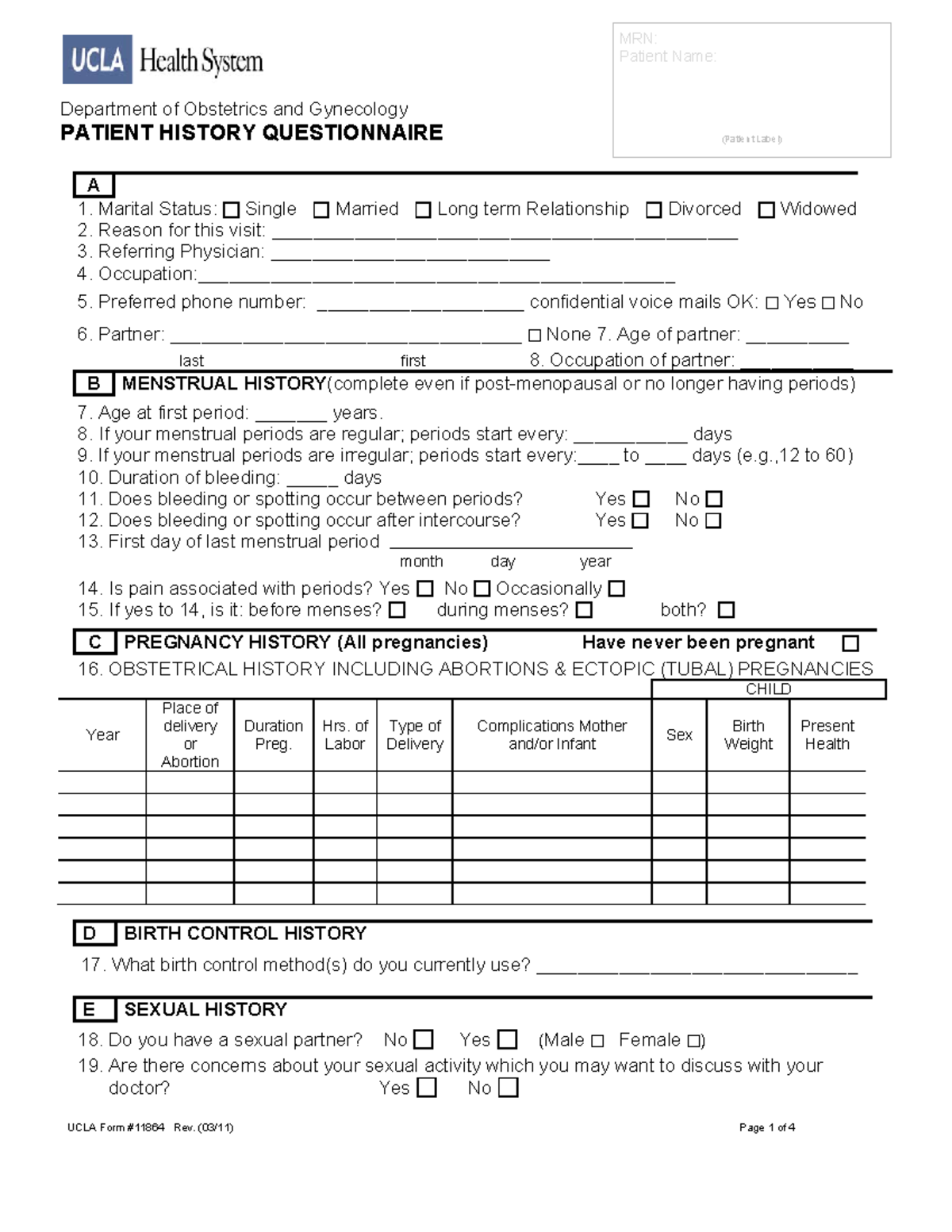
Patient History obgyn Department of Obstetrics and Gynecology PATIENT

Ob Gyn History Template
Ob Gyn History Template
Obgyn History Template
Ob Gyn History Template

ob/gyn history and physical questionnaire Doc Template pdfFiller
Obgyn History Template
Obstetric History Taking Opening The Consultation 1 Wash Your Hands And Don Ppe If Appropriate 2 Introduce Yourself To The Patient Including Your Name And Role 3 Confirm.
(03/11) Page 1 Of 4 Mrn:
Have You Ever Been Diagnosed With A Medical Or Psychological Condition?
Gynaecological History Taking Opening The Consultation 1 Wash Your Hands And Don Ppe If Appropriate 2 Introduce Yourself To The Patient Including Your Name And Role 3.
Related Post: